
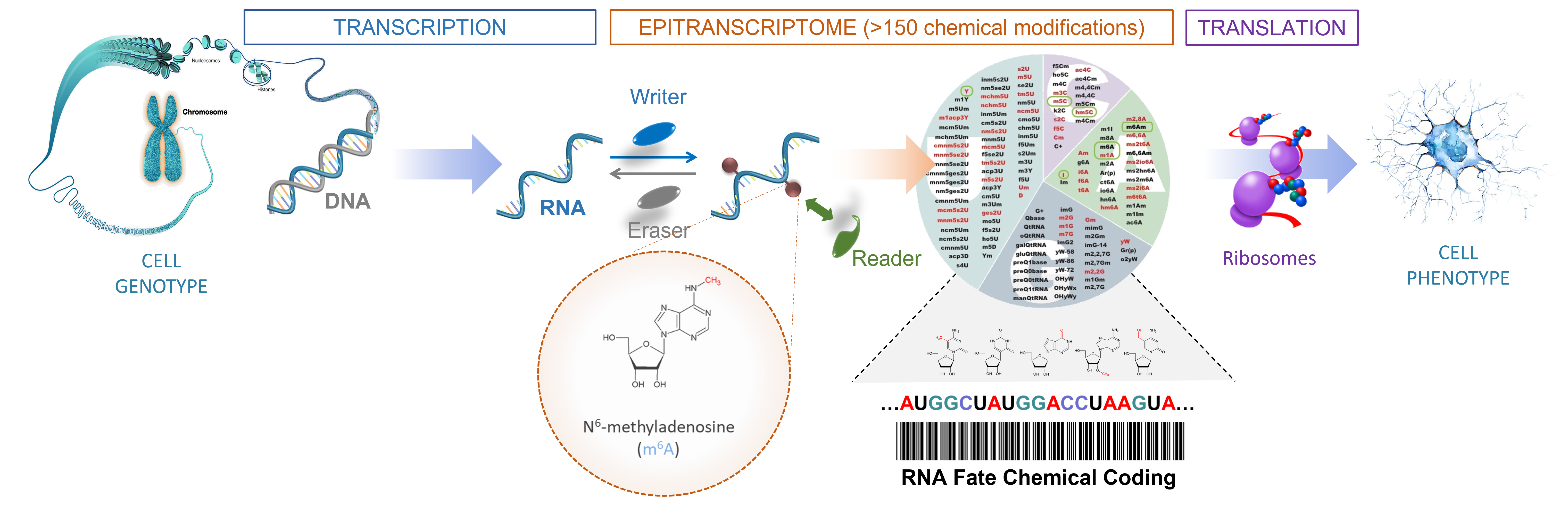
Our research work focuses on the contribution of post-transcriptional mechanisms on cancer cell adaptation, in particular RNA epigenetic & translational control.


Located in the Parc Euromédecine, the Institut de Recherche en Cancérologie de Montpellier (U1194) is located on the Val d'Aurelle Campus (ICM, Institut régional du Cancer Montpellier/ Val d'Aurelle).
U1194 Research Centre supported by Inserm, the University of Montpellier and the Institut du Cancer de Montpellier (ICM)





 Institut de Recherche en Cancérologie de
Institut de Recherche en Cancérologie de